Many Americans have heard the news account of Dr. Gregory Michael, a 56-year-old Florida physician who, after receiving his first dose of a Pfizer COVID vaccine on December 18 of last year, was hospitalized three days later. He had a total loss of his platelets — the little blood cells that stop bleeding. In spite of being treated by a team of physicians, he died two weeks later from a brain hemorrhage, and was reported to have had zero platelets. By February 10, 2021, 36 other similar cases were reported in the mainstream media. Pfizer, which along with its partner BioNTech made the vaccine the doctor received, said in a statement that it was aware of the death. Typically, they concluded, “We are actively investigating this case, but we don’t believe at this time that there is any direct connection to the vaccine.”
(Article by Lee D. Merritt MD republished from TheNewAmerican.com)
Pfizer made this “finding” despite several unusual circumstances of the case. First, low-platelet disorders, known as idiopathic thrombocytopenic purpura (ITP), most commonly affect children, and generally follow a viral illness. Only 10 percent of ITP cases occur in adults, who usually present with a slow onset form of the disorder, referred to as chronic ITP. The disorder usually starts by someone noticing easy bleeding, such as slow oozing from gums or the nose, or bruises showing up without trauma. Rarely do platelets drop below 20,000, and generally treatment either reverses the disease or prolongs life for years in spite of the problem.
What happened to this physician and the others seems to be a new previously unseen problem related to vaccination — despite the manufacturers’ claims.
Increasingly, vaccine manufacturers and government officials are following the sarcastic maxim from Samuel Shem’s novel of medical residency entitled The House of God that “if you don’t take a temperature you can’t find a fever.” In other words, if we don’t critically look at the actual recorded patient damage, we won’t find our products to be defective. Now, major media are increasingly getting on board, condemning “vaccine hesitancy” and pushing everyone to get vaccinated for COVID, discounting any dangers. But in the practice of medicine, we are supposed to employ the “precautionary principle” — above all do no harm.
Moderna and Pfizer COVID-19 “vaccines” are experimental, employing a genetic technology never before used on humans. Ironically, many people who wouldn’t purchase the first edition of a new car line are lining up to take an injection they know nothing about, that has never successfully passed animal trials, that could never meet the required “safety level” for a “drug,” and is unapproved for the prevention of COVID except as an emergency experiment.
Legally, those who get the vaccine are unnamed participants in a Stage IV FDA trial.
Moreover, a vaccine is supposed to prevent disease. By that definition, these agents are not even vaccines. They are more properly termed “experimental unapproved genetic agents.” By admission of the manufacturers themselves, both the Pfizer and Moderna products only lessen the symptoms of COVID; they don’t prevent transmission.
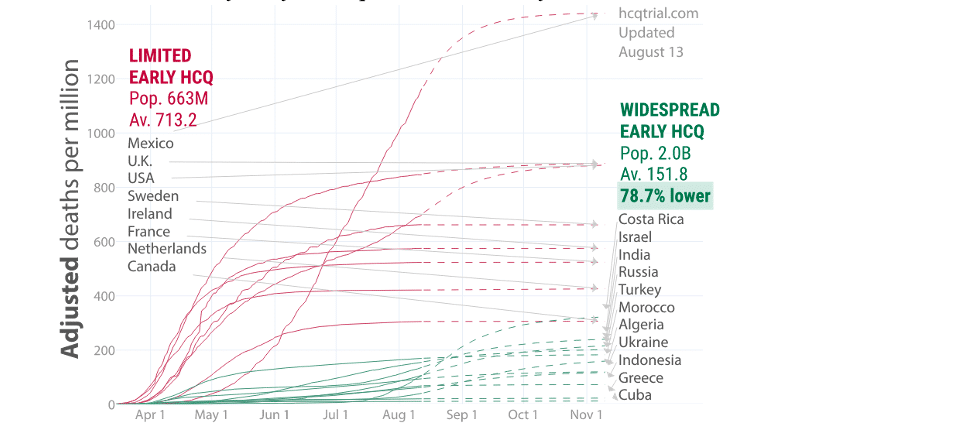
Vaccination was first invented to treat smallpox, which had a a fatality rate of up to 60 percent. Then other diseases such as typhoid and polio were similarly addressed. But vaccination is not used when effective safe treatment is available. Although censorship has confused the public understanding, overwhelming evidence dating back to the 1970s shows that viruses can be treated with “lysosomotropic agents.” The truth is, hundreds of papers have shown that chloroquine, and its later version hydroxychloroquine, are very effective in treating this virus if given early. A worldwide open architecture online review of COVID survival (hcqtrial.com) showed that death rate was 78.7-percent lower in those countries where hydroxychloroquine was used early and often:
Multiple large studies done in outpatient settings show very excellent prevention and cure with these and other drugs such as Ivermectin. In Mumbai, India, a study was done of the city police force of 10,000 officers. No deaths were recorded in the 4,600 officers taking a small dose of hydroxychloroquine each week. All the deaths were in the untreated group. Using Worldometer statistics, COVID deaths per capita in New York State are 2,656 per million population; in New Jersey they are 2,821 per million population. In India the rate is 126 per million and in Uganda it is only seven per million. Neither India nor Uganda used social distancing in any real way. But they do use hydroxychloroquine. New York (except for Dr. Zev Zelenko and a few others) does not use the drug.
As to the claims of the efficacy of the drugs, the declaration of 95-percent effectiveness of the Pfizer product was shown to be bunkum by Dr. Peter Doshi, the associate editor of the British Medical Journal, writing in that publication. After doing an independent review of the data submitted to the FDA, Dr. Doshi reported that only 30 percent of test subjects, at best, experienced even the slightest benefit (symptom reduction). Absolute risk reduction — in other words stopping transmission — he estimated at less than one percent.
The limited benefit of taking the drugs is made worse by the relatively high death tolls from the new mRNA therapy. During the first two months of the rollout of Pfizer and Moderna “vaccines” in 2021, 95 percent of deaths from vaccines recorded in the Vaccine Adverse Event Reporting System (VAERS) were for those agents, meaning only five percent of reported deaths involved all the other vaccines put together. Compared to 2019, deaths in VAERS are up 6,000 percent. Thirty-six deaths were recorded in the first quarter of 2020 versus 1,754 in the first quarter of 2021.
In Israel, where the Pfizer mRNA product is being used exclusively and a major push is on to vaccinate the whole population, an independent review of government data after two months of the vaccine program was done by the Aix-Marseille University Faculty of Medicine Emerging Infectious and Tropical Diseases Unit’s Dr. Hervé Seligmann and engineer Haim Yativ. They showed that when 12.5 percent of Israelis were vaccinated, 51 percent of the deaths from COVID were in the vaccinated group. Additionally, in the over 65-year-olds, vaccination resulted in death from COVID 40 times more than in unvaccinated people. In other words, this is not protecting people from COVID but increasing fatalities from the disease — and this neglects the number of other side effects.
If the truth were known, most sane, thinking people would not likely take part in such an experiment. With the truth hidden and with threats of travel bans and an unwarranted fear of COVID, and with pressure from employers and the politicization of COVID in general, Americans have been throwing caution to the wind.
The Unknowns
To understand what is actually happening to people after receiving the mRNA agents, I reviewed data in VAERS — an open-source searchable database of possible vaccine side effects reported by both providers and patients. According to the CDC website:
VAERS is used to detect possible safety problems — called “signals” — that may be related to vaccination. If a vaccine safety signal is identified through VAERS, scientists may conduct further studies to find out if the signal represents an actual risk.
The main goals of VAERS are to:
• Detect new, unusual, or rare adverse events that happen after vaccination.
• Monitor increases in known side effects, like arm soreness where a shot was given
• Identify potential patient risk factors for particular types of health problems related to vaccines
• Assess the safety of newly licensed vaccines
• Watch for unexpected or unusual patterns in adverse event reports
• Serve as a monitoring system in public health emergencies
The CDC acknowledges limitations of the system, including:
• Reports submitted to VAERS often lack details and sometimes contain errors.
◦ Serious adverse events are more likely to be reported than mild side effects.
◦ It is generally not possible to find out from VAERS data if a vaccine caused the adverse event.
I searched the VAERS database using keywords that would identify bleeding problems and thrombocytopenia (low or absent platelets). Entries are defined by age groups and sex with a narrative account of the injury.
In a two-and-a-half-month period from December 15, 2020 to March 12, 2021, 358 cases of unusual clotting or bleeding were identified, and it makes grim reading. There were 104 cases of frank thrombocytopenia (low platelets) — some including young people. However, the numbers alone do not adequately convey the problems. In one case about an 18-29 year-old female, the physician wrote this: “Patient was seen in in my office on 1/19/21 with complaint of heavy vaginal bleeding. A CBC was obtained which revealed an H/H of 12.2/36.1 and a platelet count of 1 (not 1K, but 1 platelet!) This was confirmed on smear review.” The surprise and horror the doctor experienced upon seeing the absence of platelets is clear when reading the report.
But the platelet problem may just be the most severe expression of a physical derangement that is producing bleeding of all sorts. As seen in the table below, there were 49 people with brain hemorrhages — nine fatal at the time of reporting. A number of other people arrived at Emergency Departments with bleeding from multiple sites, or internally, so massive that they could not be stabilized even to clearly define the sources of the bleeding.
Severe Thrombocytopenia
94
Various Spontaneous Skin bleeding
10
Mild Thrombocytopenia
11
Vein bleeding from temple
1
Thrombocytopenic Petechial rash/bruising
5
Prolonged surgical site bleeding
3
Severe Pancytopenia
2
Severe multifocal bleeding
5
Unknown Hematologic Problem
1
Severe internal bleeding
5
Multifocal or “massive” brain hemorrhage
20
Severe uncharacterized bleeding
3
Focal brain hemorrhage
29
Bleeding from cancer site liver
1
GI Bleed
34
Renal dialysis shunt
1
Severe Vaginal Bleeding
7
Hematuria
2
Vaginal Bleeding
21
Renal bleed
1
Bleeding in Pregnancy
6
Tonsillar bleed
1
Bleeding with Miscarriage
12
Acute Uterine Fibroid hemorrhage
1
Irreg Menses
4
Nosebleed
32
Oral bleeding
8
Spontaneous Splenic hemorrhage
1
Subconjunctival Hemorrhage
11
Injection Site Bleeding
21
Intraocular bleed
4
Arm Bruising
1
Most cases of severe problems were in people over the age of 50 years. But there were many younger people involved, especially in the less severe-but-unusual bleeding problems. Of the 36 reported nosebleeds, six were either unable to be stopped with usual measures, were recurrent, or were recorded as having significant blood loss or dubbed “profuse.” Many were associated with other symptoms: photophobia (eye sensitivity to light), headache, hives, “sick in bed,” brain fog, and face swelling. The youngest patient with a nosebleed was, sadly, a toddler requiring emergency care. Unusual skin bleeding was also reported. Four 65-plus-year-old males reported blood spontaneously oozing through the skin: one from the legs, one from the scalp, one from an old biopsy site, and one from an old healed “boil” site. Frank bleeding at the time of the inoculation occurred 14 times. Some bleeding was momentary, but often the bleeding was difficult to stop, recurrent, and/or persisted after the patient returned home. (How many times have you had an injection and bled at all, let alone bled off and on for hours?)
Perhaps the saddest were the bleeding episodes that preceded spontaneous miscarriages. Here are some direct entries in VAERS:
40-49 y.o. Female: The evening of my vaccination I began to feel feverish, weak and achy. During the night I woke with heavy bleeding and found out the following morning I had miscarried my otherwise healthy pregnancy.
39 y.o. Female: Internal brain bleeding 10 days after 1st dose Covid vaccine; brain damage, confused, suffering memory loss; This is a spontaneous report from a contactable physician (patient).
30-39 y.o. Female: 48 hours after injection developed micro-hemorrhages in her right eye. Symptoms resolved and 12/29 recurrence of bleeding to right eye slightly worse than before
65+ y.o. Male: Patient developed significant nose bleed after receiving vaccine. Required emergency department visits x 2 and hospitalization.
65+ y.o. Female: Vaccine administered 02/02/2021. By Thursday 2/11/2021 patient almost nonverbal, by Monday 2/15/2021 patient went to the hospital with bruising, sores on her stomach and clots reported as thrombocytopenia. Deceased by Friday, 2/19/20201.
40-49 y.o. Female: Bleeding, myalgia, tingling in the fingers of the right hand; fatigue immediately upon vaccination — bleeding at the injection site which the employee reports as filling the Band-Aid over the site. When she got home in the evening and took it off blood ran.
65+ y.o. Female: Within 15 min of the injection, the individual became aphasic and stroke like symptoms. She was taken to the ER where she was later diagnosed with a cerebral hemorrhage and passed away.
When such facts are presented, the standard retort from vaccine advocates is, “We have given millions of vaccines, so a few deaths are to be expected.” Besides the fact that a willingness to sacrifice individuals for the nebulous good of the masses represents a bankrupt moral order, simply calculating the numbers of deaths is inadequate. “Experts” need to take the time to read the narrative to open their eyes — and their hearts — to the suffering happening. There are over 25 pages of such stories printed from VAERS entries, and we must consider, “How many of these people are now dead, and how many are going to die?”
A second-year medical student armed with the facts should recognize looming disaster — where are the experts?
In truth, neither recipients nor their doctors know what is in these “vaccines.” Only a few people at the top of the Moderna, Pfizer, Johnson & Johnson, and AstraZeneca research groups really understand them. These mRNA injections produce a potentially deadly pathogen — the spike protein — in your cells. The Emergency Use Authorization for the Pfizer product says that it contains “a nucleoside-modified messenger RNA (modRNA) encoding the viral spike glycoprotein (S) of SARS-CoV-2.” If your immune system is strong enough to withstand this onslaught and create some immunity, you may survive the first onslaught. But even if you don’t die in the short term, mRNA is an epigenetic controller of DNA. Though this foreign synthetic mRNA doesn’t actually become part of your DNA to make you a “GMO human,” as some people have been worrying about, it can control DNA in ways we have yet to completely understand. We literally have no idea whether this bodily additive is going to have a side effect of expressing cancer genes, or of repressing cancer protective genes, or thousands of other potentially deadly unknowns.
Additionally, the Pfizer vaccine includes all types of ingredients that may by themselves create ailments. The Pfizer shot contains “lipids ((4-hydroxybutyl)azanediyl)bis(hexane-6,1-diyl)bis(2- hexyldecanoate), 2-[(polyethylene glycol)-2000]-N,N-ditetradecylacetamide, 1,2-distearoyl-snglycero-3-phosphocholine, and cholesterol), potassium chloride, monobasic potassium phosphate, sodium chloride, dibasic sodium phosphate dihydrate, and sucrose.”
I insert this list just for completeness — don’t expect to make sense of it. Your doctor can’t either. I understand “sucrose” (sugar) and sodium chloride (salt), but who doesn’t get lost in the “hydroxybutyl” and “distearoyl” lipid list?
After doing some sleuthing and having some inside knowledge to start from, I discovered that this lipid particle is an adjuvant called “Matrix M.” As described in scientific literature, “Adjuvant Matrix-M™ is comprised of 40 nm nanoparticles composed of Quillaja saponins, cholesterol and phospholipid.”
Matrix-M essentially wraps the mRNA in a lipid coating that allows it to move through cell walls and to linger in your system. Matrix-M is derived from plant chemicals called saponins, which have poorly understood properties in plant biology. They can be toxic to humans in some cases, and have been traditionally used by aboriginal tribesmen to poison fish. Should we consider that comforting?
The pharmacology industry has a long history of removing bad drugs from the market. Thalidomide is perhaps the most famous example of a pharmacologic disaster. The drug was released in 1957 for its sedative effects and was touted as being safe for everyone including “pregnant women and children.” In 1961, Dr. William McBride, an obstetrician, discovered that thalidomide was useful for “morning sickness” in pregnant women. Later he began to see unusual and devastating birth defects in babies born to women for whom he had prescribed the drug. Independently, Dr. Widuking Lenz, a pediatrician in Germany, also associated thalidomide with severe and unusual birth defects, such as the absence of limbs or parts of limbs. Sometimes an infants’ hands were attached at the shoulders, there being no connecting long bones at all. By 1962 the drug was taken off the market.
But unlike with our new, experimental agents, recognition of the thalidomide problem was made relatively easy by several factors. First among these was the uniqueness of the deformities. These were both profound and obvious, which stand in stark contrast to the current bleeding problems, which appear on the surface to be normal problems in clinical medicine — such as nosebleeds. Even now, doctors continue to call the loss of platelets “ITP” — even though what we are seeing is not the same as what we would expect to see under that diagnosis. ITP simply does not kill adult males in a few days.
Second, with thalidomide, the physician who first began using the drug for nausea in pregnancy was also the doctor who delivered the affected babies, so he could readily put two and two together. In the case of our COVID drugs, when your doctor tells you to get a vaccine, he doesn’t administer it, doesn’t witness the injection, and usually doesn’t follow up to see how you fared. And if you were to suddenly develop a vision problem or bleeding from the bowel, you wouldn’t be seen by your PCP; you would be in an Emergency Department — and they don’t usually ask about your recent vaccine history.
Third, Dr. Lenz presciently recognized that, in the case of thalidomide, many less-severe deformities, when put into perspective, revealed “gradations of the defect.” Unfortunately in the present case, lesser degrees of clotting problems are indistinguishable from bleeding issues frequently encountered in an Emergency Room or doctor’s office. For example, if a 75-year-old hypertensive male — who has gotten a COVID shot — suffers a brain hemorrhage and dies, it would not likely be deemed unusual, and the relationship to vaccination may not even be explored.
Keeping that in mind, we should assume the worst when it comes to these new COVID shots. When any new drug problem starts, it begins slowly and unrecognized — like a snowball beginning to roll down a mountain. By the time the problem is generally acknowledged, the avalanche is well on its way. In the case of thalidomide, over 100,000 children were severely damaged before the drug was removed from use. Though VAERS has the potential to shorten recognition time of drug problems by trying to spot the “unusual patterns,” this requires that physicians be aware of the system, and take the time to enter any suspected side effects — not just the worst cases. It also requires that researchers care enough to look. This is not happening. A report previously submitted to the Agency for Healthcare Research and Quality revealed that fewer than one percent of adverse events get reported to VAERS.
In the past, testing done on mRNA technology revealed problems specifically involving the clotting system. Antibody-mediated platelet damage has been suspected. Yet today when these exact problems arise, the researchers are mum. Do the experts not study or know their own vaccine research history?
For those who are concerned about the risks, we need to advocate for ourselves, either through contacting legislators or simply refusing to take the shots. It’s obvious that the pharmaceutical industry is willing to release untried technology upon the entire world population, and not be deterred by any inconvenience such as unexplained death.
We need to stop being a gullible population that forces our children to get vaccinated for trivial, non-fatal diseases such as mumps. We need to stop believing in the god-like status of medical technocrats who claim to be making the world safer. We need to reject the idea that vaccine deniers are anti-scientific troglodytes. We must reject the unspoken premise under which pharmaceutical companies and doctors operate — that all vaccines are always safe in all people all the time. It should not be considered unreasonable to require scientific transparency, honesty by drug manufacturers, and safety from vaccines.
Vaccines are only indicated for diseases with a high risk of death or morbidity, and for which there is no cure. After seeing the esteemed leaders in medicine denigrate hydroxychloroquine (even though it was a recognized treatment used successfully elsewhere for SARS, and mentioned favorably by Dr. Fauci for MERS), after watching three plants used in the production of hydroxychloroquine burn down in a year — two on the same day — after watching doctors lose their jobs and be censored for speaking truth and saving lives with old safe drugs that work, and now, after seeing experimental genetic agents being rolled out for use globally that have never passed animal testing and have only a few months human trials, perhaps it is time to address the 800-pound gorilla in the room and ask, “Are they trying to kill us?”
Read more at: TheNewAmerican.com
All content posted on this site is commentary or opinion and is protected under Free Speech. Citizens.news is not responsible for content written by contributing authors. The information on this site is provided for educational and entertainment purposes only. It is not intended as a substitute for professional advice of any kind. Citizens.news assumes no responsibility for the use or misuse of this material. Your use of this website indicates your agreement to these terms and those published on this site. All trademarks, registered trademarks and servicemarks mentioned on this site are the property of their respective owners.
 Parler
Parler Gab
Gab