 Parler
Parler Gab
Gab
How Many People Are Killed by Psychiatric Drugs?
If we want to estimate the death toll of psychiatric drugs, the most reliable evidence we have are the placebo-controlled randomised trials. But we need to consider their limitations. First, they usually run for only a few weeks even though most patients take the drugs for many years.13,14 Second, polypharmacy is common in psychiatry, and this increases the risk of dying. As an example, the Danish Board of Health has warned that adding a benzodiazepine to a neuroleptic increases mortality by 50-65%.15 Third, half of all deaths are missing in published trial reports.16 For dementia, published data show that for every 100 people treated with a newer neuroleptic for ten weeks, one patient is killed.17 This is an extremely high death rate for a drug, but FDA data on the same trials show it is twice as high, namely two patients killed per 100 after ten weeks.18 And if we extend the observation period, the death toll becomes even higher. A Finnish study of 70,718 community-dwellers newly diagnosed with Alzheimer’s disease reported that neuroleptics kill 4-5 people per 100 annually compared to patients who were not treated.19 Fourth, the design of psychiatric drug trials is biased. In almost all cases, patients were already in treatment before they entered the trial,2,7 and some of those randomised to placebo will therefore experience withdrawal effects that will increase their risk of dying, e.g. because of akathisia. It is not possible to use the placebo-controlled trials in schizophrenia to estimate the effect of neuroleptics on mortality because of the drug withdrawal design. The suicide rate in these unethical trials was 2-5 times higher than the norm.20,21 One in every 145 patients who entered the trials of risperidone, olanzapine, quetiapine, and sertindole died, but none of these deaths were mentioned in the scientific literature, and the FDA didn’t require them to be mentioned. Fifth, events after the trial is stopped are ignored. In Pfizer’s trials of sertraline in adults, the risk ratio for suicides and suicide attempts was 0.52 when the follow-up was only 24 hours, but 1.47 when the follow-up was 30 days, i.e. an increase in suicidal events.22 And when researchers reanalysed the FDA trial data on depression drugs and included harms occurring during followup, they found that the drugs double the number of suicides in adults compared to placebo.23,24 In 2013, I estimated that, in people aged 65 and above, neuroleptics, benzodiazepines, or similar, and depression drugs kill 209,000 people annually in the United States.2 I used rather conservative estimates, however, and usage data from Denmark, which are far lower than those in the US. I have therefore updated the analysis based on US usage data, again focusing on older age groups. For neuroleptics, I used the estimate of 2% mortality from the FDA data.18 For benzodiazepines and similar drugs, a matched cohort study showed that the drugs doubled the death rate, although the average age of the patients was only 55.25 The excess death rate was about 1% per year. In another large, matched cohort study, the appendix to the study report shows that hypnotics quadrupled the death rate (hazard ratio 4.5).26 These authors estimated that sleeping pills kill between 320,000 and 507,000 Americans every year.26 A reasonable estimate of the annual death rate would therefore be 2%. For SSRIs, a UK cohort study of 60,746 depressed patients older than 65 showed that they led to falls and that the drugs kill 3.6% of patients treated for one year.27 The study was done very well, e.g. the patients were their own control in one of the analyses, which is a good way to remove the effect of confounders. But the death rate is surprisingly high. Another cohort study, of 136,293 American postmenopausal women (age 50-79) participating in the Women’s Health Initiative study, found that depression drugs were associated with a 32% increase in all-cause mortality after adjustment for confounding factors, which corresponded to 0.5% of women killed by SSRIs when treated for one year.28 The death rate was very likely underestimated. The authors warned that their results should be interpreted with great caution, as the way exposure to antidepressant drugs was ascertained carried a high risk of misclassification, which would make it more difficult to find an increase in mortality. Further, the patients were much younger than in the UK study, and the death rate increased markedly with age and was 1.4% for those aged 70-79. Finally, the exposed and unexposed women were different for many important risk factors for early death, whereas the people in the UK cohort were their own control. For these reasons, I decided to use the average of the two estimates, a 2% annual death rate. These are my results for the US for these three drug groups for people at least 65 years of age (58.2 million; usage is in outpatients only):29-32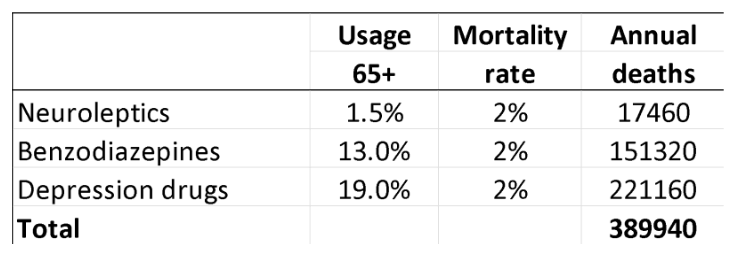


Colombia CUTS diplomatic ties with Israel over genocide of Palestinians in Gaza
By Ramon Tomey // Share

UNMAS: There is more war debris in Gaza after seven months than in Ukraine after over two years
By Laura Harris // Share

Beijing warns Washington against crossing “red lines” to avoid CONFRONTATION
By Belle Carter // Share

NHTSA probes Tesla’s recall of 2 million cars over Autopilot concerns
By Ava Grace // Share

NIH defies FOIA, Moderna vaxx royalties paid to government remain state secret
By News Editors // Share

No Deal on Iran: Why the West's Unreasonable Demands Will Lead to Global Catastrophe
By healthranger // Share


These 4 antioxidants could be the missing link for tired, dull skin
By isabelle // Share

Humanoid robots enter American homes as Gatsby launches autonomous cleaning service
By isabelle // Share


Modest curcumin dose shows blood sugar improvement in older prediabetic adults
By isabelle // Share